01 Overview
Replacing a 20-year-old case-management system used by nurses at a US health insurer.
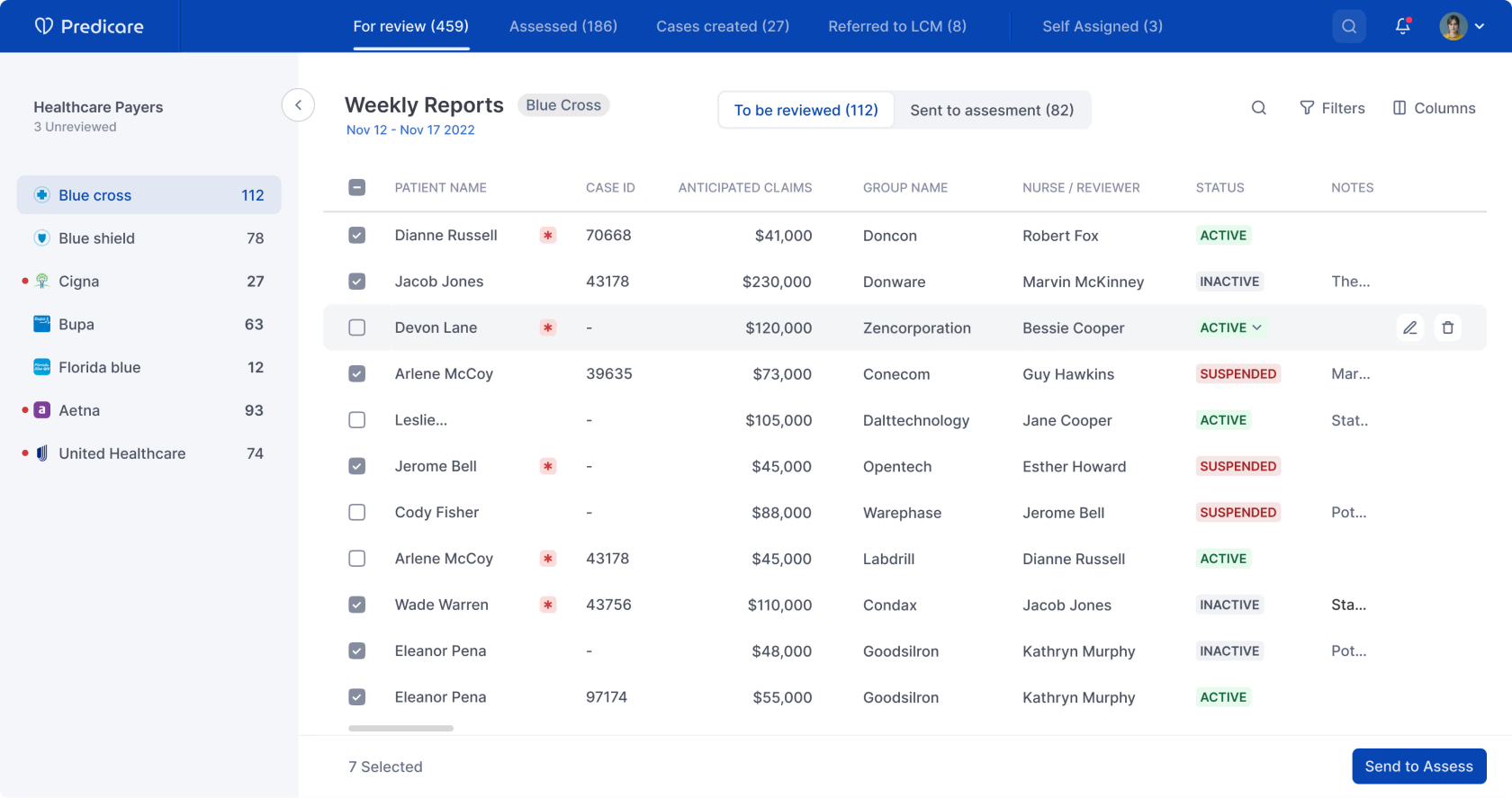
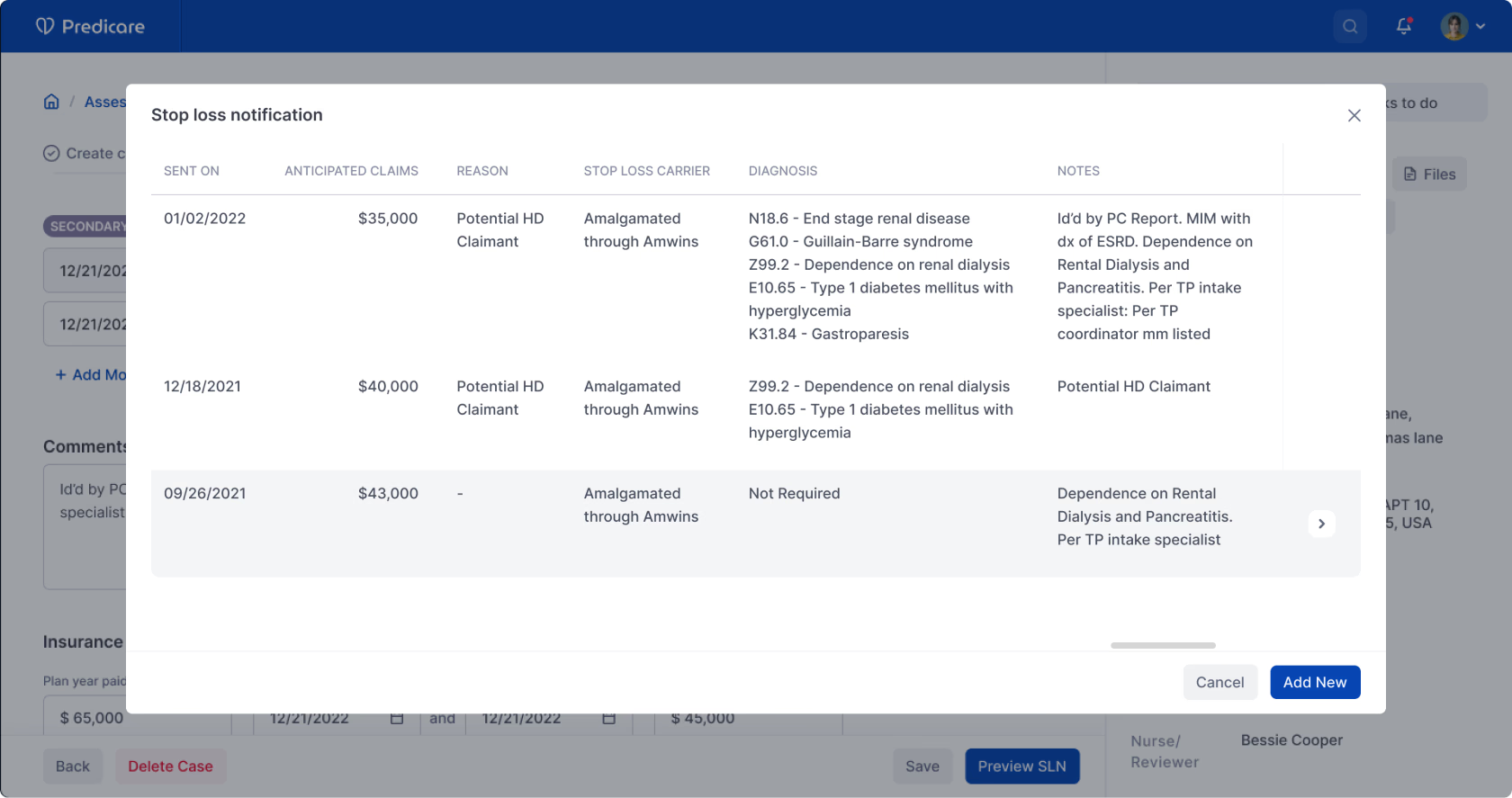
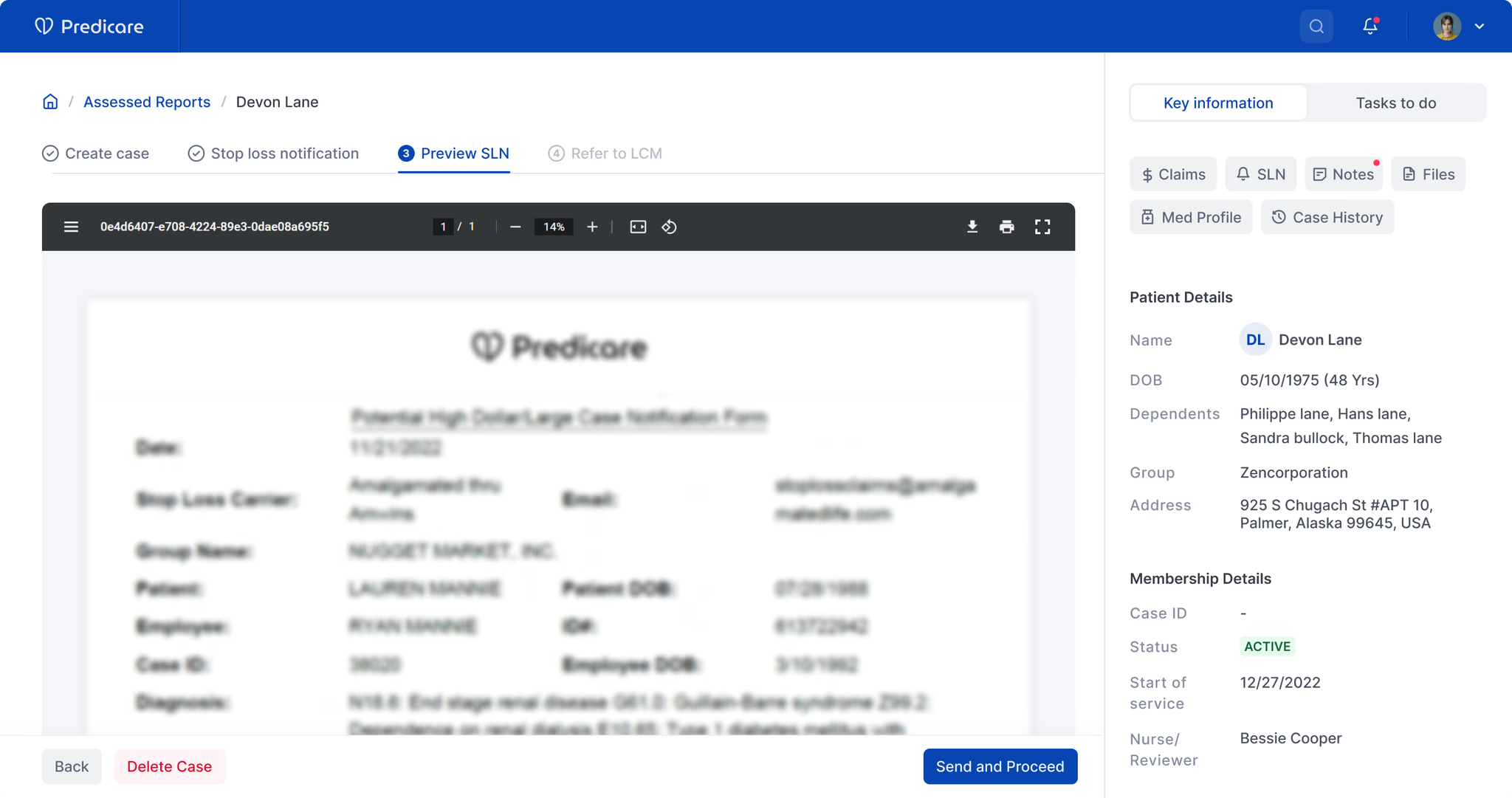
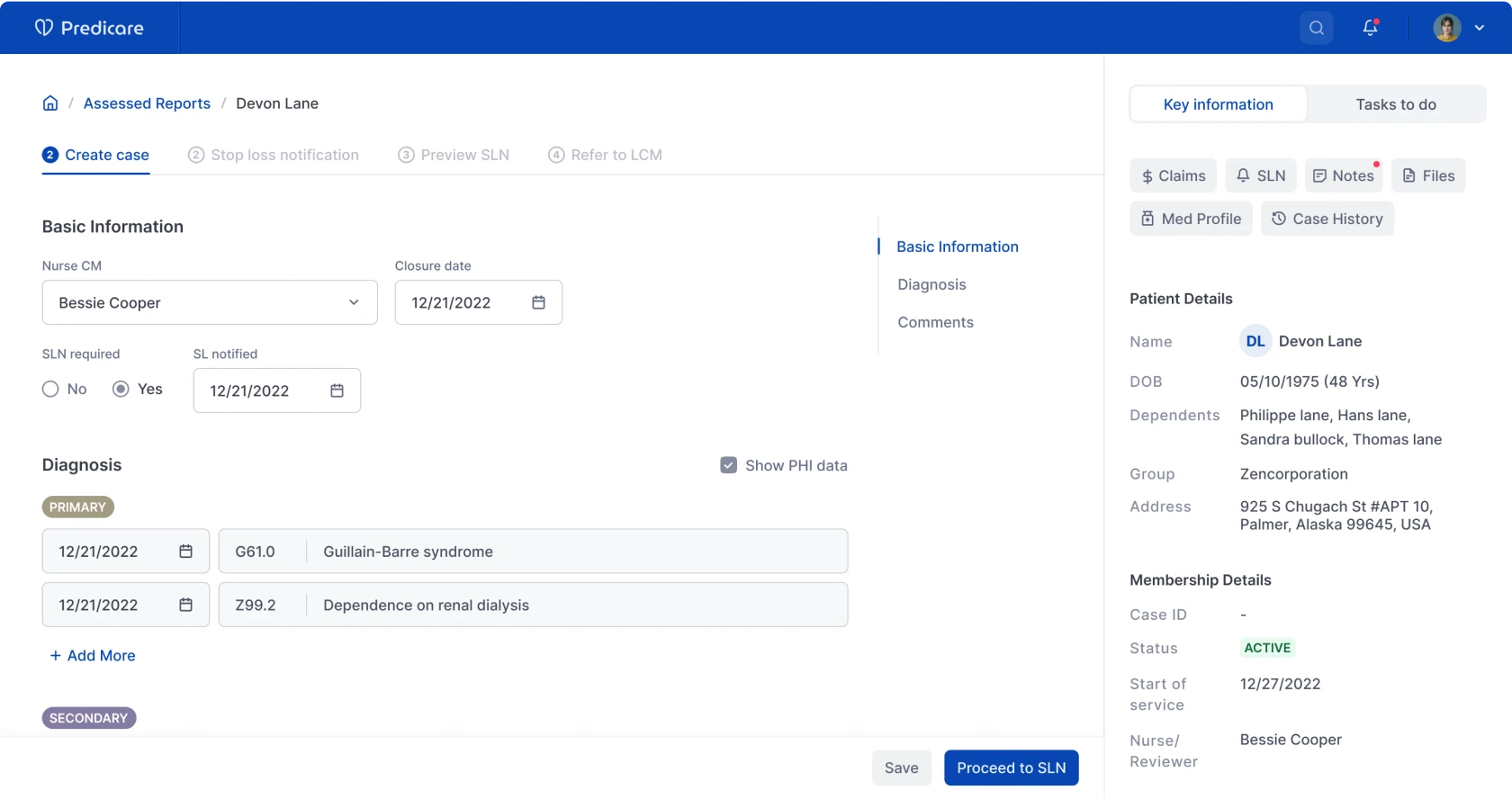
Predicare is a platform US health insurers use to help their back-office nurses catch serious health issues in members early — before the member ends up back in hospital. AI sits in the background doing two jobs: managing the health-plan paperwork, and flagging claims that look fraudulent.
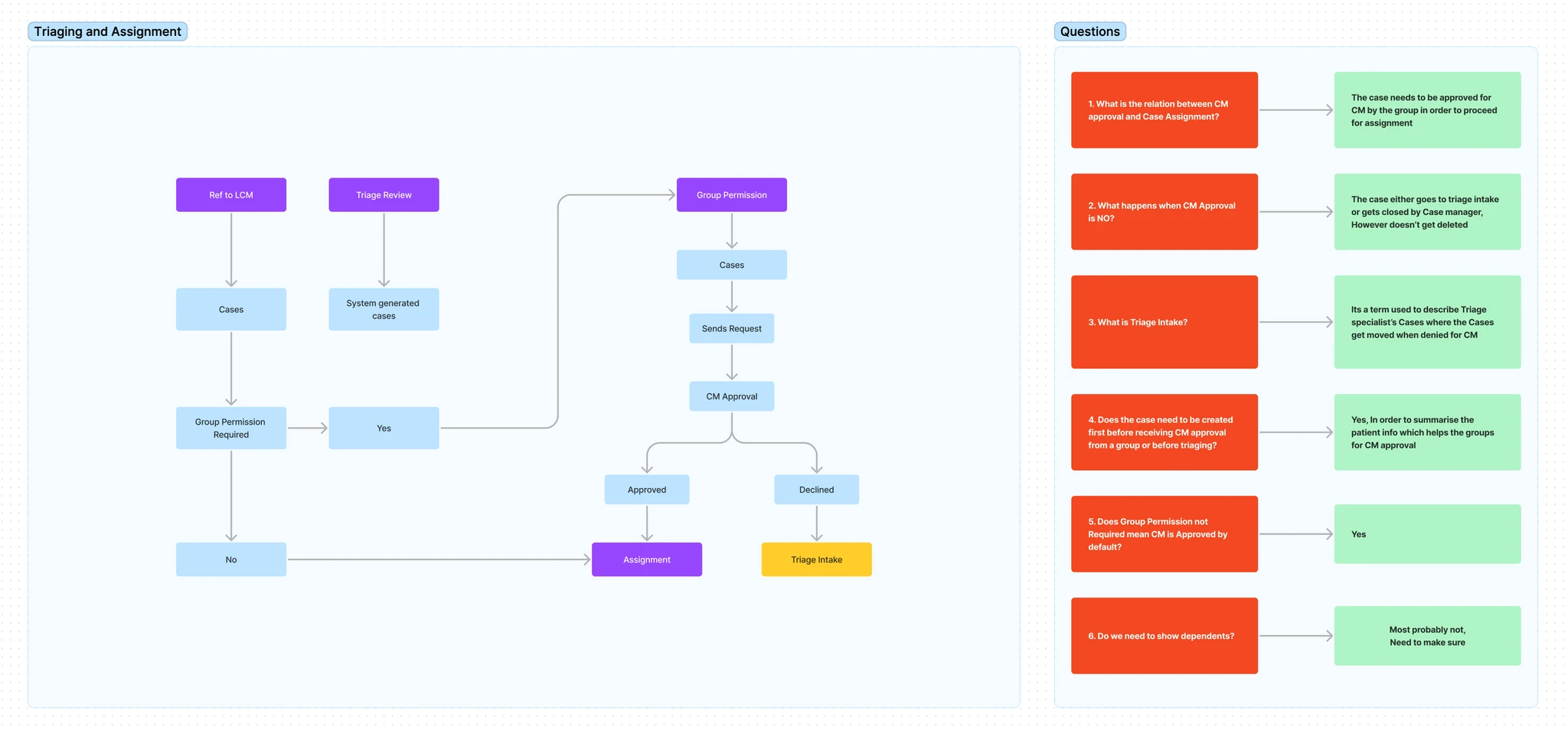
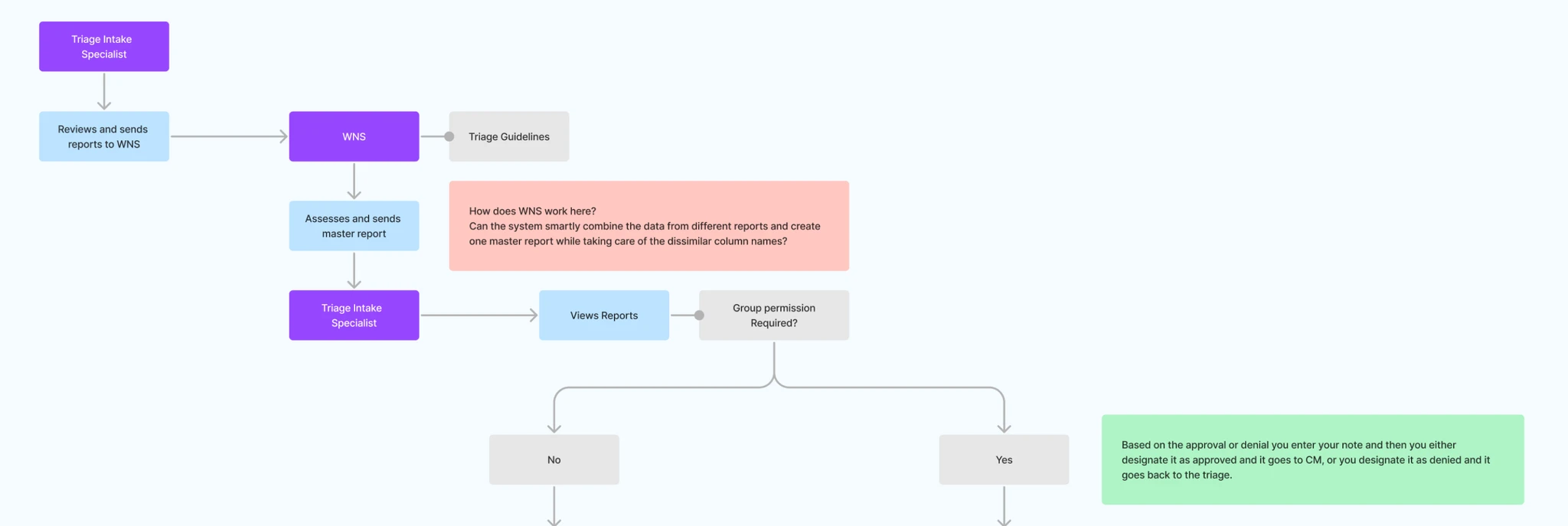
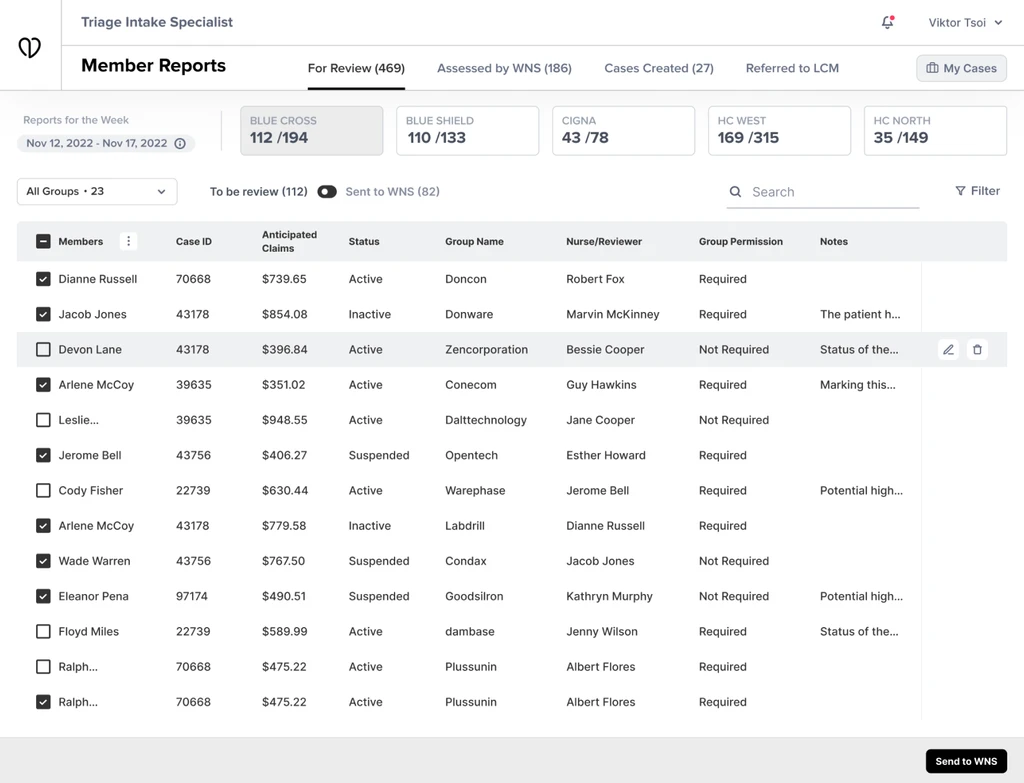
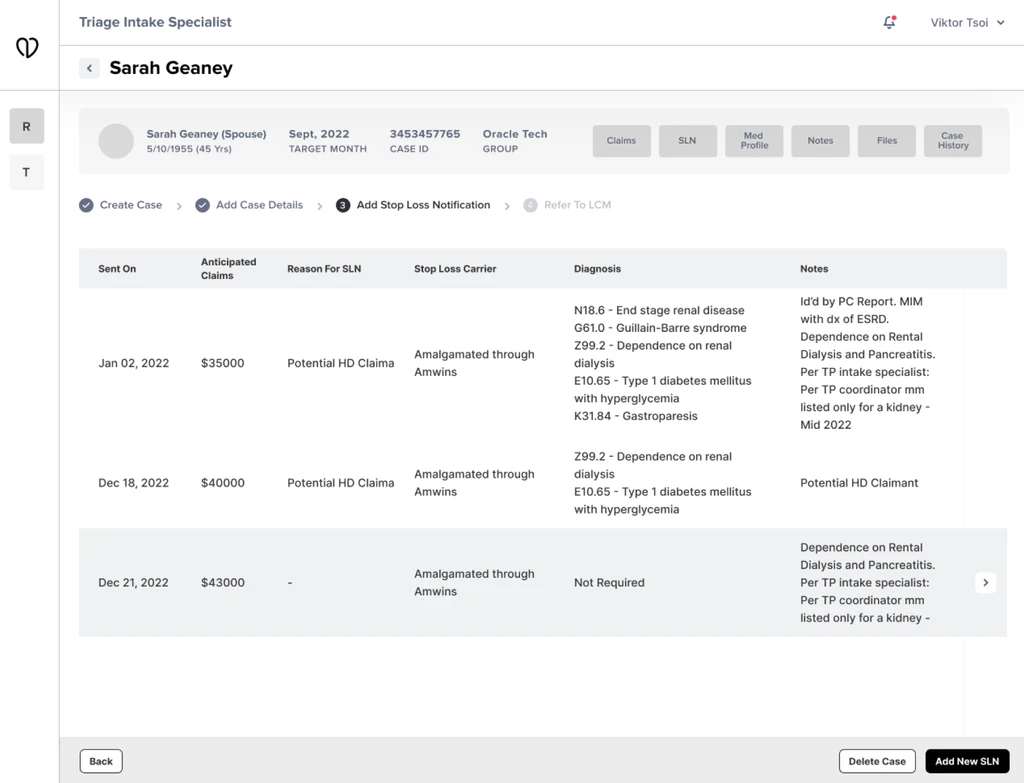
Three designers were working on the rebuild of the original system, which had been built in the early 2000s. This case study covers the bit I owned: the workflow nurses use to open and run a patient case.